THE PRODUCTION FUNCTION OF HEALTH
A production function summarizes the relationship between inputs and outputs. The study of the production of health function requires that we inquire about the relationship between health inputs and health. The answers that economists and medical historians offer to this question surprise many people. First, the contribution of practitioner-provided health care to the historical downward trends in population mortality rates was probably negligible at least until well into the twentieth century. Second, while the total contribution of health care is substantial in the modern day, its marginal contribution in some cases is small.

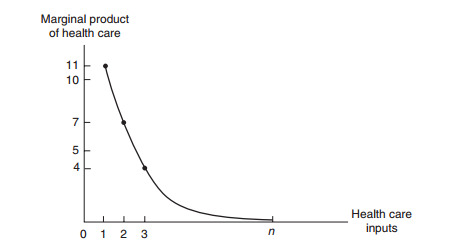
To simplify the depiction, we have reduced all health care inputs into one scale called Health Care. In reality, health care consists of many health care inputs. Some of them include medical care provided by doctors of medicine or osteopathy, but other health care professionals also provide care. Conceptually, the health care measure, HC, may be thought of as an aggregate of all these types of health care, the aggregation being based on dollar values. The marginal contribution of health care is its marginal product, meaning the increment to health caused by one extra unit of Health Care, holding all other inputs constant. Increasing Health Care from zero to one unit in Figure 5-1A improves health status by ΔHS1, the first unit’s marginal product. Numerically, this first unit of Health Care has increased the health status index from 32 to 43; ΔHS1 = 11 Health Status units. The next unit of medical care delivers a marginal product of ΔHS2 = 7, and so on. These marginal products are diminishing in size, illustrating the law of diminishing marginal returns. If society employs a total of n units of Health Care, then the total contribution of Health Care is the sum of the marginal products of each of the n units. This total contribution as shown, AB, may be substantial. However, the marginal product of the nth unit of medical care is ΔHSn, and it is small. In fact, we are nearly on the “flat of the curve.” Marginal product is graphed on Figure 5-1B. We have drawn the health production function as a rising curve that flattens out at higher levels of health care but never bends downward. Would the health production function eventually bend downward? Is it possible to get too much health care so that the health of the population is harmed? This is a logical possibility under at least two scenarios. Iatrogenic (meaning provider-caused) disease is an inevitable by-product of many medical interventions. For example, each surgery has its risks. Combinations of drugs may have unforeseen and adverse interactions. If the rate of iatrogenic disease does not fall while diminishing returns sets in, it is possible for the balance of help and harm from health care to be a net harm. Medical scientists, such as Cochrane (1972), have pressed the case that much medical care as often practiced has only weak scientific basis, making iatrogenesis a real probability. Writing for the public audience, Dubos (1960) and Illich (1976) once warned of a medical “nemesis” taking away our abilities to face the natural hardships of life by “medicalizing” these problems. Illich argued that this medicalization would lead to less personal effort to preserve health and less personal determination to persevere; the result becomes a decline in the health of the population and thus a negative marginal product for medical care.2 Return to the distinction between total product and marginal product. Often, the marginals, rather than the totals, are relevant to policy propositions. For example, no one seriously recommends that society eliminate all health care spending. However, it is reasonable to ask whether society would be better off if it could reduce health care expenditures by $1 billion and invest those funds in another productive use, such as housing, education,
transportation, defense, or other consumption. We could even reasonably ask if health itself could be improved by transferring the marginal $1 billion to environmental or lifestyle improvements. Many of our government programs encourage health care use in certain population groups, such as the poor and elderly. Other programs, such as tax preferences for health insurance, provide benefits for those who are neither poor nor elderly and encourage their consumption of health care. The theoretical issues raised here suggest that we question the wisdom of each of our programs. The theoretical questions can be investigated with data of several kinds either directly or indirectly relevant to the production of health issue. We begin with the historical role of medicine, which indirectly bears on the issue of health production. After providing an overview of these efforts, largely the work of medical and economic historians, we then turn to econometric studies of the modern-day production function.
